Institutionalizing the Insane in Nineteenth-Century England
By Anna Shepherd
Studies for the Society for the Social History of Medicine 20
Pickering & Chatto, 2014
HB 978 1 84893 431 3: £60/$99
eBook: £24 (incl. VAT)
On a prime 150 acre site in Surrey at Woking, Brookwood Asylum opened its doors on June 17, 1867. Established by the Metropolitan Asylums Board, it was the second public county asylum at Wocking, created to deal with the overflow of patients from the first Surrey County Asylum, Springfield (est. 1841).[1] Eighteen years later and ten miles away, in another month of June, the Holloway Sanatorium invited the middle-class to its resort for rest and recovery from a variety of mental ills. Set up by private bequest, Holloway was designed to cater exclusively to the middle-class insane; it even relied on fees from wealthy patients to subsidize less affluent patients who were still considered “deserving” of assistance.
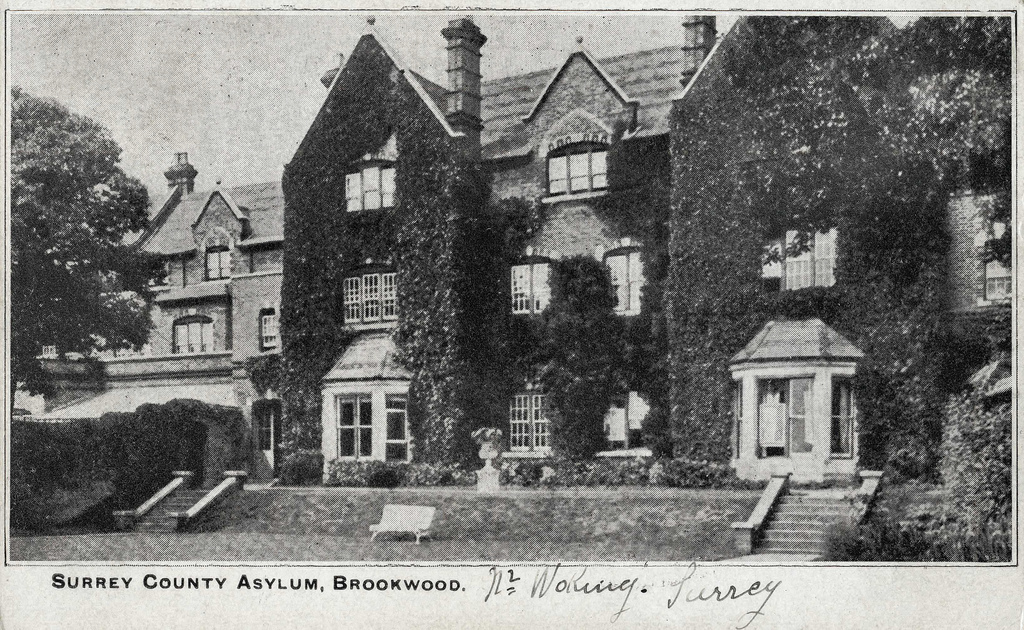
Brookwood County Asylum

Holloway Sanatorium. Wood-engraving from the Illustrated London News, 5 January 1884
Anna Shepherd’s Institutionalizing the Insane in Nineteenth-Century England traces the history of these geographically close, but ideologically distinct institutions. Relying on an abundance of archival materials, including asylum reports, admission registers, case books, hospital rules, drug books, and patients’ correspondence, Shepherd’s empirical study challenges the stereotype of nineteenth-century asylums as madhouses or dumping grounds, especially for victimized women. Particularly challenging the assumption that women were disproportionally incarcerated in the nineteenth century, Shepherd argues
The rationale behind [the institutions’] establishment suggests that contemporary class perceptions shaped their existence and management. Class defined committal and discharge processes and, combined with contemporary expectations of appropriate behaviour for men and women, influenced diagnosis, treatment and outcomes.
The influence of class is particularly evident in the architecture and designs of the institutions. Brookwood was designed to be cost-effective and largely self-sufficient; its rural location provided the capacity to establish farms where patient could grow their own food and where staff could govern refractory patients. Plain and functional, with minimal decorations, the entire asylum functioned as a therapeutic effect. With no excessive decorations to distract patients or for staff to maintain, the plainness of the asylum contributed to treatment concentrated on the “moral management” of patients’ minds.
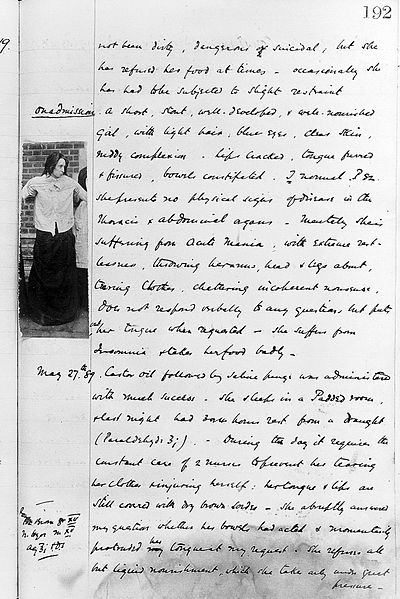
Holloway Sanitorium case notes for Constance Coddingto, 1889 (Wellcome Library)
The Holloway Sanitarium, other hand, concentrated on beauty and luxury in order to maintain the rigid class distinction of Victorian life—even if design led to an oversight of some basic legal requirements, such as not having a chapel built in the original architectural plans as stipulated by law. Demand for private mental care advocated by families concerned for afflicted relatives and a growing medical interest in the links between insanity and hereditary disorder, led to the sanatorium employing features of upper-class lifestyle. Physical labor, for instance, was not appropriate for the majority of patients. Rather, patients were encouraged to participate fully in varied recreation activities, social events, and entertainment programs. However, some patients were encouraged to work in order to combat idleness, considered as dangerous to the therapeutic process. Nor were Holloway patients confined strictly to institutional grounds; for therapeutic value of fresh air, during the summer months patients could stay at rental coastal properties (37).

A “band promenade” at Holloway Sanatorium, c.1905 (Surrey History Center)
The strength of Shepherd’s thesis resides in her analysis of the rich sources of personal correspondence between families of patients that indicate a variety of circumstances and reasons for the incarceration of relatives in the asylums. At Brookwood, most patients were transferred from workhouses, another asylum, or removed from their own homes; occasionally, children were admitted, usually brought by their patients. Records describe physically ill, dirty, malnourished, and neglected individuals, some arriving to the institution with clear evidence of mistreatment. Few were beyond help. While the asylum did not take private patients, families or friends concerned by workhouse conditions of their loved ones, or simply overwhelmed with home care, brought patients to Brookwood. As Shepard notes, this incarceration process was incredibly traumatic, and relatives often expressed concerns about the eventual discharge of their family member. One letter to the Brookwood superintendent, by the husband of Caroline W, admitted August 27, 1867 in a maniacal state with a breast infection, expresses this concern (72):
Dear Sir, I was verrey sorrey to hear that my wife Caroline Walsh was taken so Bad I hope it will not be for long Please God her Babey is getting on as well as can be exepectted with the mother I hope yo will be kind and to let me know when she is likely to be fit for home.
Please do remember me to my wife and give my kind love to her.
I remain yours truly, Thomas Walsh.

The female ward at Brookwood Asylum, 1881 (Surrey History Center)
At Holloway, on the other hand, the majority of patients came from their own homes as relatives and friends concerned with the behaviour of their relatives admitted them to the sanatorium. Families and friends were especially involved and influential over commitments and discharged of their relatives. Other patients were transferred from other private institutions, but interestingly, a sizable number were “voluntary boarders” or uncertified patients (75). The voluntary process clearly accorded with middle-class sensibilities as voluntary patients were essentially free agents, and being uncertified, they could escape the stigmatization of being certified. Instead, their stay at Holloway functioned as a temporary refugee from the stress and perils of life; they were allowed to take a break, recuperate and recharge their mental sensibilities to full health. Doctors also believed that voluntary admission positively assisted the recovery process as patients were more relaxed, allowing staff to make a more accurate diagnosis; for some voluntary patient, Holloway became such a safe haven that they remained there as boarders (106). Once in a while, a criminally insane member of the middle-class was admitted to Holloway, such as John W. who was admitted in 1887 after being diagnosed with suicidal mania after slitting the throat of a sixteen year old servant (76).
The medical staff acted as agents of care, deciding therapeutic regimens of their patients accordingly to diagnosis. Diagnosis was not standardized. Rather, the medical staff made their assessments as influenced by class and gender perceptions as well as evidence provided by families and friends. Causes were usually attributed to classified diseases dementia, mania, melancholia (which accounted for nearly a third of all admissions to Brookwood), intemperance, hereditary insanity, worry, and anxiety. Patients were especially admitted to mental worries related to gender expectations: male patients who were expected to deliver wages were strained when they felt they failed to uphold their obligations. Anxieties and disappointment of love were also causes. For the majority of cases, regardless of social class, treatment resided on moral therapy, occasionally supplemented by physical activity, surgery (at Brookwood), and a broad range of chemical (including opiates) and electric treatments. At Holloway, innovative therapies were used, such as massage and gym exercise. Restraint methods, such as the “dry-pack” was also used to deal with troublesome and maniacal patients at Holloway; at Brookwood, seclusion was especially beneficial for dealing with violent outbursts in order to protect staff and other patients. However, medical staff were particularly cautious in using seclusion to deal with suicidal patients; as Shepard points out, suicidal patients often found creative ways to achieve their tendencies, so the control of suicidal behaviour was considered by medical staff as an indicator of therapeutic success.
Institutionalizing the Insane provides fantastic window into the lives and worries of nineteenth century people. Shepherd describes how reasons for incarceration were not always rooted in serious mental illnesses; in some instances, everyday worries were enough for individuals or their families and friends to seek out medical care. Statistical evidence, considered by nineteenth century institutions as a reliable measure of effectiveness, adds another dimension to Shepherd’s analysis.[2] Numbers revealed how medical history, circumstances, and treatments were all perceived as indicators of treatment success, while still highlighting the importance of family interactions and expectations. A solid study, this book will surely appeal to those interested into the complex lives and treatments of the insane during the nineteenth century.
NOTES
[1] The Metropolitan Asylums Board was created to care for the infectious and insane poor of Greater London.
[2] For instance, Brookwood had high death rates, sometimes 15% of all admissions in a given year. While environmental issues, such as overcrowding and inadequate water certainly played a part, Shepard argues the asylum’s high intake of physically weak and chronically ill patients from the workhouses surely contributed to the death rates.


Latest Comments